
Welcome to my second installment on red light therapy dosing. I've previously created the red light therapy dosing chart - part I of this endeavor - wherein I showcase all the recommended dosing protocols based on high-quality previous research.
In this blog post I explore the massive implications of that earlier work. I take more of a philosophy of science approach in this blog post about why dosing is complicated, and why there may not be a super simple and elegant formula that optimizes dosing for everyone.
Nevertheless, I still argue that earlier recommendations on this topic work reasonably well for most people. I also give you an introduction to how red light therapy dosing is normally calculated and related basic terms and definitions.
If you just want to understand the basics of this topic, check the summary I've included below. If you want to read individual sections in more detail, check the table of content on the left. And if you want full understanding, just read the entire article!
In this blog post, I make the case for several reasons that red light therapy dosing is complicated and that there's no universal simple answer. In other words, there's no simple formula that's 100% optimal for all human beings under every circumstance.
And yet, I do think that the original "standard model" of red light therapy dosing - developed by Ari Whitten as far as I know in his 2018 book - is a great heuristic and tool for people to start their dosing journey.
So here's how you start:
You first check how much light your red light therapy device is emitting through our shopping tool. You'll get a figure measured in milliWatt/cm2 (mW/cm2) measured 6 inches from the device. You multiply that mW/cm2 by each second you treat yourself, and divide by 1,000 to reach the Joules/cm2 dose that's applied on a given area.
You don't need to understand the full technical details of that formula, just need to use it. The dose here that's often recommended of up to 15 J/cm2 for superficial tissues and 60 J/cm2 - the "standard model" - is a great starting point for many. From there, you can experiment with a higher or lower dose.
The J/cm2 is how much red light therapy per day you should generally use. So if you ask "how long is a red light therapy session" - it all depends on the dose you're trying to achieve.
From a more scientific perspective, however, and my reflections on that science, it's a lot harder to achieve a universal dosing calculator that's correct for each circumstance in humans. I give many different reasons especially later on in this blog post why I think it's unlikely that we'll find a very simple and elegant formula, like the ones are available in physics, such as "E = mc2", because the human body is an organism ruled by complexity theory and not by simple mechanistic movements.
In plain English, that means that your individual health circumstances and context may dictate the red light therapy dose. For instance, your overall health, tolerance to light in general, nutritional status and many other factors likely affect how red light therapy dosing works for you.
My work is not of pure skepticism and doom and gloom, however. Instead, I think the standard guidelines formulated for superficial tissue treatment of up to 15 J/cm2 and 60 J/cm2 for deep tissue treatment is a great place to start for many. From that setpoint, you can likely experiment through trial and error and find out what works for you.
The Problem With Red Light Therapy Dosing: Searching For The Perfect Formula
In an ideal world, you'd have very simple formulas to understand very complex phenomena. Physics is a great example thereof. Almost 350 years ago, Isaac Newton published his laws of motion:
1) A body remains at rest, or in motion at a constant speed in a straight line, except insofar as it is acted upon by a force.
2) At any instant of time, the net force on a body is equal to the body's acceleration multiplied by its mass or, equivalently, the rate at which the body's momentum is changing with time.
3) If two bodies exert forces on each other, these forces have the same magnitude but opposite directions (1).
The second law, for instance, can be easily understood as "F = m * a", or Force (F) equals mass multiplied by acceleration. Later on, that formula turned out to be a special case within a broader framework, whereby Einstein would account for the speed of light in relation to time at higher velocities. Space and time are merged for Einstein and give rise to another formula that is:
E = mc² (2)
I'm not a physics expert myself but I do understand the elegance of these equations. From a simple equation, you can device a lot about this world. Now, ideally, you'd have the same in red light therapy. And we have the same in red light therapy, in a way, because we've got simple formulas for calculating a dose - I'll explain more about these in a second:
mW/cm², applied over time in seconds divided by 1,000, equates to a dose in Joules/cm² (my own phrasing of the formula!)
Next up, you have a simple dose for superficial and deeper tissue treatment. Ari Whitten has laid out this formula best in my opinion, in his great 2018 book on red light therapy, has laid out this formula best (3; 9).
I think as a basic tool, that formula works really well for most people. But, the formula is not without flaws in my opinion, or at least, the red light therapy dosing chart that I've created at least questions whether there should be 2 independent universal dosing formulas for superficial and deeper tissues.
I know Ari personally and he's an absolutely wonderful person, so this is not an attack on him in any way. I just think, after spending a few weeks going through the research, that we're not in a situation where we can create a simple formula, like Newton or Einstein did, that's adequate for all of human biology.
But, let's first look into what that formula is, created by Ari Whitten a few years ago, that gave us very simple and elegant dosing parameters for superficial and deeper tissues:
The Original Red Light Therapy Dosing Calculator
Getting the dosage right on red light therapy is essential. Some studies actually find no results from red light therapy when using the wrong dose (or light frequencies).
That outcome should not come as a surprise.
An analogy with exercise is great to understand this principle: if you use an exercise intensity that's too low or too high, you won't get the results you're aiming at. The same is true for red light therapy.
At the most basic level, just one thing matters for achieving the right dosage: the amount of "Joules" of red and infrared light hit that your skin over time.
Sounds complicated? Let's dissect that sentence...
What are "Joules"?
Joules are a unit of energy. Under the classical model of red light therapy dosing, we want an intensity between 3 and 60 Joules per square centimeter (cm2) of your skin for almost all treatments. That's more or less the consensus on the internet, and in the science.
The higher the Joule value, the more light energy you're thus adding to (a specific part of) your body.
Knowing your Joule input takes some effort. You generally have to do some calculations to arrive at that Joule value.
Most red light devices supply you with a milliwatt per square centimeter (mW/cm2) dosage of light.
In general, the milliwatts per second you're exposed to increases when you get closer to a red light therapy LED panel and decreases the farther removed you're from a red light therapy device.
That milliwatt per square centimeter number can be used to calculate a Joule value. For every 1,000 mW/cm2 added to your body, 1 Joule (per cm2) is added.
Let me give an example:
A red light therapy device might add 20 milliwatts per square centimeter per second, or alternatively, 100 milliwatts per square centimeter (per second). In the first case, it takes 50 seconds to add 1 Joule of energy to your body--in the latter case, it only takes 10 seconds.
Let me give you a simple analogy to understand red light therapy dosing:
Knowing how many Joules (per square centimeter) is like knowing the weights you're using in the gym: if you use three times as much weight, the effect will be very different.
Let's do some calculations to better understand the concept of "Joules":
- Let's say you want to put 50 Joule of energy into your body. Your red light device puts out 100 mW/cm2 per second at a 50-centimeter distance.
Every minute you use the device would add 60 seconds * 100 mW/cm2 = 6.000 mW/cm2 = 6 Joules of energy (per square cm2) to your body.
When rounded-off, you need to use your red light therapy device for about 8 minutes to get a dosage of 48 Joules. - Let's say you want to put 20 Joules (per cm2) of energy into your body. Your red light device puts out 10 mW/cm2 per second, at a 100-centimeter distance.
In one minute, you'll put about 10*60 = 600 mW/cm2 into your body, which equals 0,6 Joules (per cm2). For 20 Joules, you would need 20 / 0,6 J = 33,3 minutes of therapy - which is a long time.
Solution?
Move closer to your device. At a 20 centimeter distance, the device might put out 100 mW/cm2. From that distance, you'll add 6 Joules of energy per minute, which would equal 3,3 minutes of total treatment.
The latter case sounds much better right? - Let's say you want to do a skin treatment, and need to put 5 Joules of total energy into your body. The skin is a very superficial organ and does not need very high dosages.
Assume that you've got a big light panel that puts out lots of light.
You're standing at a 30-centimeter distance, and you're thinking: "10 minutes ought to be enough to get great results!"
Big mistake...
Let's calculate:
At a 30 centimeter distance (~12 inches), the light output is 90 mW/cm2. That distance and light output combination equal 5.400 mW/cm2 or 5,4 Joule per minute. If you're using your device for 10 minutes, you're adding a total of 54 Joules of energy to your body, which is more than ten times the amount of energy you needed for skin treatment (5 Joules).
Big mistake!
You're using the red light therapy panel totally wrong. With 54 Joules, you're treating your deeper tissues, while not getting an effect in your skin at all.
I cannot repeat that principle often enough: you need the right dosage for any specific goal you may have. But, as you've already seen in part I of my red light therapy dosing guide, where I give a chart, that the numbers vary wildly for different goals.
To know what you're doing, you need to calculate the dosage.
Fortunately, many companies nowadays do supply a dosage guideline with their product, so that you don't need to go through these calculations manually. The bad thing is, however, that most of these calculations are wrong - something I'll explore in the next section!
Sometimes, companies offer a simple app to calculate the dosage - which is a great development, although, usually imperfect.
I've decided to include this section anyway because you might not have such a manual, or you might have a light setup where you combine several red light therapy panels.
Let's now look at how to treat different tissues...
Even though that topic of dosage seems complicated, it's really not:
- More superficial tissues, such as your skin, teeth, or superficial blood vessels, need a low dosage of 3-10 Joules
- Deeper tissues, which include your muscles, joints, organs, or bones, need between 20 and 60 Joules. Most studies actually stay around the 20-40 J dose, every few days.
But these are averages, and for the science-backed dosing guidelines for different goals, check my earlier dosing chart.
Once you go over 80-90 Joules, you generally reduce the overall red light therapy effects. If you surpass 20 Joules, moreover, you'll also decrease the treatment effects for superficial tissues, but increase the effects on deeper tissues (although I'm oversimplifying here, more on this later!)
Oh yeah, one more thing:
This bears repeating: always keep in mind that your red light therapy device is often accompanied with a description of its light output at a very specific distance.
Always take that distance into account. While going off the input of companies isn't perfect, it's better than doing nothing - the perfect is the enemy of the good here.
Better yet, use our own Shopping Tool to know the quantity of mW/cm2 you're getting at 6 inches.
Again, if you get closer to the device, of course, the mW/cm2 per second will increase, upping the total Joules per cm2 of energy that are added to your body.
In terms of dosage, the amount of light you need can vary from person to person. The maximum dosage of 60 Joules per square centimeter is not set in stone for everyone.
Why?
You may remember that I've treated the concept of "hormesis" in a previous blog post on stress. Hormesis entails that the right intensity of a biological stressor could make your body stronger, while either too low or too high of a stimulus has adverse effects.
If you're in poor overall health, using red light therapy might mean that you would need a lower overall dosage, to begin with.
While I've just given a maximum dosage of 60 Joules, if you've got a disease such as fibromyalgia or Alzheimer's, you'd want to start off with a much lower dosage. After testing a low dosage, watch how your body reacts. If treatments are successful, you may be able to increase your dosage over time.
The same principle applies to other "hormetic stressors" I've talked about before, such as cold therapy or exercise.
If you've read my cold blogs in the past, you'll remember that I'm recommending people easing very slowly into cold therapy. Just as too much intense exercise makes you more tired, and too much cold therapy makes you more tired (or worse: gives you frostbite or hypothermia), red light therapy has the same effect.
I personally know people who have chronic pain or fibromyalgia who are wiped out by doing too much red light therapy!
That's all you need to know?
No, not yet...
Lastly, even though you can do multiple red light therapy sessions per day, I would not exceed 60 Joules per cm2 each day. Staying closer to 40 J is probably even better.
That recommendation entails you can do two treatments of 20 Joules per day or one treatment of 40 Joules per day.
I would also lower the overall dosage if you're spending lots of time in the sun.
Why?
There's no need for a 60 Joule dosage if you've spent 3 hours in the sun. If you're spending that much time in the sun, it's better to use a 5-10 Joule treatment to optimize your skin condition.
The good thing? You now know about the basics of dosing red light therapy. The bad news? Things are more complicated than the basic calculations I've just carried out above - here's why:
Red Light Therapy Dosing: 8 Reasons Why It's Complicated
So, below I'll tell you why the original red light therapy dosing calculator oversimplifies in many different areas. I don't have a simple solution here, besides telling you that for most people, the model is great. Except, in the future it may turn out that there will be better data available for many instances!
Below I've listed a few reasons for my conclusion:
Reason 1: Studies On Many Topics Haven't Tested For Many Variables Yet
So I've discussed this topic very extensively in my last blog post where I laid out the red light therapy dosing chart. Here's what I mean:
Let's say there are 30 studies on red light therapy for goal X. These 30 studies use the wavelengths of 405 nm, 450 nm, 560 nm, 630 nm, 810 nm, and 850 nm. In that case, what can you say about whether 590 nm light works, or 830 nm, or 1,064 nm, if there's no data on that topic?
You can't say whether a wavelength works without testing! And if you'd say that 1,064nm doesn't work, that's simply a wrong statement - the correct statement is that there's no data on whether 1,064 nm light works for goal X.
The same is true for many different variables on many different topics:
- If different power outputs haven't been tested for, you don't know whether these power outputs work or not.
- If different treatment areas haven't been tested for, you don't know whether different treatment areas work or not.
- If different treatment areas haven't been tested for, you don't know whether that treatment area being affected works or not.
- If different combinations of wavelengths haven't been tested for, you don't know whether these combinations work or not.
I'll make a simple analogy here to prove my point:
- If you've tested someone for their zinc status, and their copper status, you don't know about their magnesium status. To know about their magnesium status, you'll have to test for their magnesium status explicitly (such as a red blood cell test).
- You can know about someone's hand grip strength and their VO2 max, but you don't immediately know their 40 year dash from these numbers. Maybe there are indirect implications from VO2 max and especially hand grip strength for sprinting speed, but you don't know for sure what their 40 yard dash is!
So, back to red light therapy - here are some examples once again:
- Let's say there are three studies on a given goal X. Study 1 uses 40 mW/cm2 full body, at 660 nm with LEDs for a total dose of 12 J/cm2, study 2 uses 200 mW/cm2 for 5 J/cm2 at 810 nm, and study 3 uses 100 J/cm2 at 100 mW/cm2 at 630 nm. In that case, you don't know which of these protocols is superior. You also don't know whether 60 mW/cm2 works better than 40 mW/cm2 or 100 mW/cm2, because that study isn't available. You also don't know whether 630 nm, 660 nm, or 810 nm is superior for goal X because the wavelengths haven't been tested against each other.
- Next up, for Alzheimer's, let's say there are two studies with a transcranial (through the skull), with 250 mW/cm2 on the prefrontal cortex for 3 minutes at 810 nm, and 125 mW/cm2 at 810 nm for 3 minutes. In that case you don't know whether the same parameters at 1,064 nm would have the same effect, because it's not tested for. Let's say there's a third study, with a 1,064 nm helmet that emits 10 mW/cm2 and is to be used for 10 minutes. If there's no other study with a 1,064 nm helmet, at 20 mW/cm2 that's used for 5 minutes, you don't have the data on which protocol is superior of the two, using helmets.
- And so forth. The topic is extremely complex because we're missing tons of data on different treatment parameters, and also on comparisons between parameters.
Reason 2: Study Setups Vary Wildly From Each Other
Overall, study setups are very different from each other, making universal dosing guidelines almost impossible. Let's take Alzheimer's Disease as an example - Vladimir Heiskanen's Excel Sheet contains about 90 studies on Alzheimer's Disease right now.
Some of these studies use transcranial devices, while others use intranasal devices and others use more of a cap-shaped device (or a helmet). The studies also use different wavelengths, although there's a preference for near-infrared light.
And, even if say a transcranial device is used, it's placed at different points of the skull. Then, there are wildly varying power outputs across studies. And, there are different participants in these studies, such as healthy participants, those with mild cognitive impairment, and those with full-blown Alzheimer's Disease - all of which probably need different treatment.
Reason 3: Study Quality Varies Big Time
Now, it gets even more complicated than this. If you really want to know the dosing for each of these goals, you'd have to read the individual studies and rate them on their merit. Normally, this is ideally done during a systematic review, and I'm assuming here that the reviews have done so correctly, which is not always the case.
A systematic review analyzes previous studies on a topic, ranks these studies, and then integrates the evidence. So, let's say, there are 20 studies on red light therapy for knee pain (I'm just making that number up), the review would include these studies on the topic, rank them on bias, and then tell you based on the studies how good the evidence on red light therapy for knee pain is.
In an ideal world, we'd only be doing systematic reviews, for each topic out there. But creating a good systematic review takes at least a few weeks of full-time work (and up to months), not even including the peer review process and publication. As we're a company and cannot rely on tax dollars, writing systematic reviews is simply not a possiblity for us.
But, to truly understand dosing for each goal, such as muscle recovery or treating Parkinson's Disease, you'd have to read all the individual studies yourself and rate each study on its own merit, such as the risk of bias, funding, and so forth. As we're a for-profit company and don't have government funding to spend a few weeks on exploring each topic in great detail, that option is not available, unfortunately.
If you'd really want to do a perfect or extremely good job, you'd have to spend 20-40 hours per topic - such as Alzheimer's Disease or Parkinson's - and get a much better answer on red light therapy dosing. You'd have to rate all studies on the topic, check all their protocols in great detail, calculate the effect sizes for all studies, and then give out a few recommendations per topic.
Maybe in the future, once I have a research team! For now you'll have to do with my imperfect red light therapy dosing chart that's arguably still the best out there right now!
Reason 4: Data In Individual Studies Can't Even Be Relied On 100%
Now there's another issue that James Carroll has talked about: many researchers in the photobiomodulation space don't report their treatment parameters perfectly, or don't measure their devices perfectly, or just use a device because that's what's available for research, without looking at the alternatives.
We live in an imperfect world, but ideally, you'd check and double and triple-check all your parameters before making a publication. Some publications, however, don't even list the J/cm2 dose or the mW/cm2 dose.
If you're curious, check out James Carroll's interview here with Alex Fergus, which touches upon the methodology in research in part:
Most of these conclusions come from private conversation with James Carroll, however.
Reason 5: Study Participants Have Different Results With Different Dosing Parameters - As Do People In The Real World
People respond slightly different to red light therapy. We've all known this observationally, by looking at how different people respond to, say, red light therapy panel or mask treatments.
Some people will do great with a 70 mW/cm2 dose, or even a 200 mW/cm2 dose with a big panel directly pressed against the skin (me). Others are far more sensitive to light and can only handle a few minutes per treatment area at 30 mW/cm2.
So at what treatment parameters people get benefits also varies from person. But the same is true for side effects. If you've got chronic illness, for instance, such as fibromyalgia, or metabolic syndrome, heart disease, and a neurodegenerative disease combined, you may want to take it easy in the beginning!
Even Michael Hamblin now states explicitly that there seem to be differences between people, on how they respond to red light therapy in the following interview (at the 27:17 mark):
Here's the transcript:
Interviewer: And, how about the dose-response curve, I'm aware that it's not a linear curve - there is a point of diminishing returns. So, how if you were to use one of these panels, how were you to know what the minimal effective dose is, and what the best dose is?
Hamblin: Right, so the thing that confuses people even more than you just mentioned is that different people respond differently. Some individuals are highly sensitive to light [next words not audible]. Some individuals are like blocks of wood, shining light on them all day and nothing will happen.
The majority are in between, it's like a Bell Curve [comment: Gaussian distribution, with 68% of the people found between 1 standard deviation from the mean].
It is the hypersensitive individuals that will most often complain that they've got adverse effects from photobiomodulation.
And your question of, how do you know woh these hypersensitive individuals then the answer is, well they're hypersensitive, they complain about all sorts of things you know, they're allergic, they don't like loud noises, they don't like bright light, they can only eat certain kinds of foods.
You know, their whole life seems to be governed by being hypersensitive. So if you're going to treat these people with photobiomodulation be very careful because they're the ones that complain about all sorts of things going wrong.
You know, the majority in the middle, and it's difficult to overdose them on light. I'm not saying you can't do it. You know, most people - and it's not a sudden drop off, right - most people can figure it out by trial and error.
And if they think, well, you know, I've got some benefit, you're kind of constrained by the lengts of time it's going to take. But there again, you can get a more powerful device. So if you have a 2 Watt LED device, for instance, and you use it for 15 minutes, good, that's nice.
And you use it for 30 minutes, and it's better, and eventually what you're going to do is get a more powerful device so you don't have to spend 3 hours laying under this device.
So, yes, most people can figure that out for themselves.
Keep in mind these aren't mine words. Nor, do we have strict evidence for that dosing protocol from scientific studies, in my opinion - and if you do, can you please comment on this post and show me these studies?
Reason 6: Many Of The Studies Don't Use Full-Body Panels Or Beds
Many of the studies I've cited are carried out on small areas, with lasers, which give a different outcome (most likely) than for full-body treatment!
There have only been a few LED panel studies so far, and a few with red light therapy beds (mostly the NovoTHOR).
Ideally though, you'll want more studies with LEDs, especially bigger panels, to know how people respond differently to them. I know I've covered this point in part in reason 1, but still, I think this topic needs an independent place because it's coming from a very different perspective.
Reason 7: We Don't Know Whether Wavelengths Interact
So here's another brain problem for nerds:
What if wavelengths interact, and combining wavelengths changes the effect that therapy has?
For instance, what happens when you add a decent dose of Ultraviolet-A to your regular mix of 630 nm, 660 nm, 810 nm, and 850 nm? Ultraviolet-A affect nitric oxide in the cell, which then affects blood flow (7; 8). The change in blood flow, theoretically, may alter the effects of the red and near-infrared light.
Maybe the Ultraviolet-A light even extends the systemic effects that red and near-infrared light have, because of the improved blood flow. Again, all of this is speculation, because I don't have the data on this. And until you and I have data on this topic - and these conditions are tested for - you cannot say that you know for certain what will happen in these circumstances.
That's simple logic 101...
Also, what happens with blood flow, or reactive oxygen species, or the mitochondrial effects, or cytokines related to inflammation, when you add blue light to red and near-infrared light? Or when you add green light, or both?
Again, I don't know the answer here because I cannot find good data on this topic!
Reason 8: Different Dosing Methods, Such As The Contact Method Or Non-Contact Method Yield Different Results
Andrew LaTour has talked about the contact method of red light therapy extensively in the past. I've not done a deep dive into the research on this topic myself, so I'll have to stay agnostic, but I will say from personal experience is that even with higher-powered panels, I seem and feel better results with the contact method myself.
Assuming Andrew is correct here, the results will change for all of the variables I've discussed above as to whether a contact method is applied or not, with panels or other devices, for the results. The amount of reflection and penetration depth will vary big time, with or without the contact method - the argument of LaTour goes!
Why Dosing Is Likely Complex, And There Is No Easy Answer
So let's make a bit of a detour here. I'll try to explain why red light therapy dosing is potentially so complicated and why there are no easy answers.
One of my most memorable statements pertaining to the philosophy of science is that of Immanuel Kant in 1970. Kant stated that:
"There will never be a Newton of the blade of grass” (4).
In Kant's work that contains that quote, The Critique of Judgement, he distinguishes between mechanisms and organisms. Mechanistic thinking applies to objects in nature such as sand, rocks, and planets, while organism applies to biological creatures at the very least.
For instance, a rock you let fall of a tower is relatively simple to analyze, even with Newtonian mechanics. You have clear inputs, use the Newtonian laws of motion, and you'll have clear outputs.
But for biological organisms, and many other complex phenomena, simply applying laws to the inputs to get clear outputs doesn't work. Let's explore why. Wikipedia describes this difference well:
" such as living beings, whose parts exist for the sake of their whole and their whole for the sake of their parts. This allows him to open a gap in the physical world: since these "organic" things cannot be brought under the rules that apply to all other appearances, what are we to do with them" (4).
That's where we end up with modern complexity theory. Complexity theory or chaos theory is what describes such phenomenon in today's terminology. Examples here are financial markets or the weather - there are many parts of the system that are influenced by each other and mutually influence each other. There's no simple cause-and-effect relationship, as there is with dropping a stone from a tower such as in the Newtonian laws of motion.
(Human) biology is similar. Examples here are that your organs' functioning is interdependent - your heart cannot function without your lungs and vice versa. The neural network in the brain interacts through billions of cells, which indirectly interact with the food you take in, but then also again determine how you access food. Cells depend on how atoms and molecules function in your body, but your functioning as an organism as a whole again determines the state of the atoms and molecules.
Everything mutually presupposes each other - without a clearly defined beginning and end. Not only are there many variables in health, all of these variables also affect each other.
I therefore don't think we'll find a super short and elegant formula that describes how dosing should work, for all people, in all potential circumstances, in just two sentences. Here are some of the implications of this problem:
- Below I've posted an example of a citric acid and electron chain transport test - from the NutrEval lab test (6):
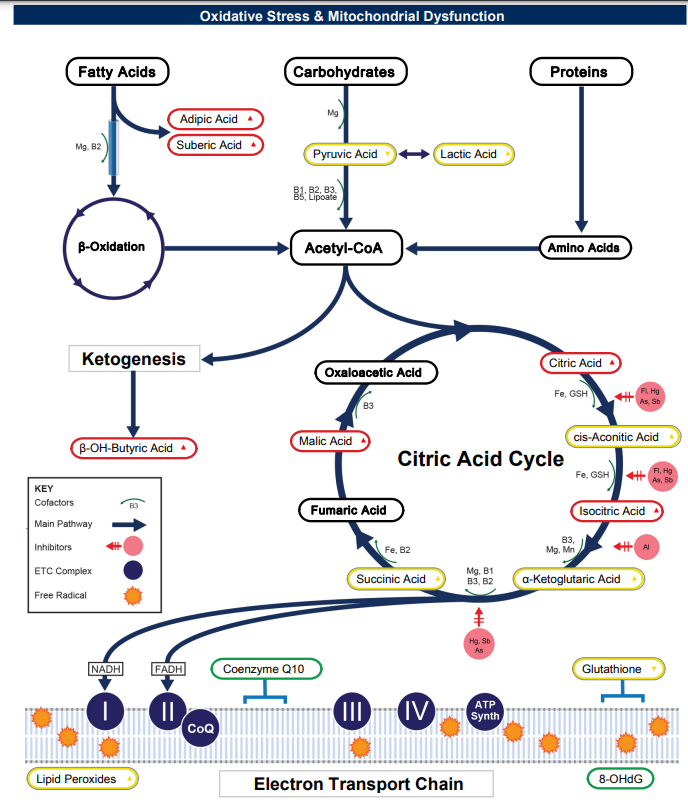
- That test seems complicated but what's most important to remember is that for each of these steps, for the energy-production process in the body, certain vitamins and minerals may be necessary and toxins such as mercury or arsenic limit energy production.
- The question here is, are you certain that with the same input of light (so, let's say, full body treatment with LED panels, at 50 mW/cm2, for a total dose of 30 J/cm2), the results will be the same for each person? Of course not, because you don't know the exact nutrient status and even toxicology status of each individual. If a person has mercury or arsenic poisoning, some steps of the energy-creation process will be compromised, and light may have different effects for both individuals. Once more, you don't know for sure without testing!
- We also already know that many different factors influence how you respond to red light therapy. Skin type, for instance, and gender affect the response. But what if there are many more other variables that affect the outcome? What if the iron in your blood affects the systemic effects of red light therapy? What if the amount of sleep you got last night(s) influences the results? What if with different meal timing, your red light therapy results change?
So What's Next? How to Monitor And Adjust Your Dosing
The solution? In my opinion, trial and error works really well. Michael Hamblin already alluded to that solution earlier, and my good friend Alex Fergus has done the same recently, in a video about red light therapy dosing:
The solution here isn't nihilim–but trail and error instead! You can still measure how well you're doing with red light therapy and without, and with different treatment parameters for yourself and observe what you're responding to well.
If you respond well to a protocol, use it and experiment with more or less of it until you find a sweet spot. If a protocol doesn't work, change things up - it's that simple!
Red Light Dosing Guides for Specific Conditions and Goals
If you still want to follow the exact science on this topic, just check my red light therapy dosing chart. There you'll find the current best evidence of dosing protocols for many different goals, based on systematic reviews (which have the highest level of evidence in medical science).
Conclusion: A Red Light Therapy Dosing Calculator Is Still An Enigma!
I wish it were simpler. And I wish I could give you a simple red light therapy dosing calculator that's universally true for all circumstances and does justice to all individual circumstances.
Here's an analogy:
In fitness, there's been a long discussion whether sets of 8 repetitions, 10 repetitions, or 12 repetitions are superior for mass gains. And then there's the discussion of whether you need 1 set of 8 repetitions, 2 sets of that number, or three, or even more.
There too, there's probably not a universal answer that is correct for every individual. If there were, study participants would respond exactly the same in scientific studies on these topics.
Nevertheless, for optimal dosing, and if you want to be 100% science-based, you'll have to follow the red light therapy dosing chart numbers and ensure the device you're using is following these numbers. Of course, with more data emerging over time, I fully expect these numbers to change over time!
Frequently Asked Questions
Below I consider a few frequently asked questions about red light therapy dosing:
What If You Get Too Much Red Light?
If you get too much red light (or near-infrared) your results will decline and eventually may even become negative.
While some stimulus is good, more is not always better. Think about it, if you're training for the marathon, running two or three times per week at moderate intensity is great for your improvements. But if you'd run at maximum intensity six days a week, your results drop off quickly and the speed at which you complete a marathon would decline.
Red light therapy is the same - some red light therapy is good, a bit more is better, but if you continue increasing the dose you'll impeded and finally get negative results.
Does The Red Light Therapy Distance Matter?
Sure, the distance of the red light therapy device to your skin matters. The greater the distance, the lower the dose arriving at your skin.
If you want a great approximation of how distance affects the red light therapy dose, check Alex Fergus' wonderful videos on the red light therapy treatment area of one panel, and the treatment area with multiple panels.
What Is The Red Light Therapy Wattage?
Wattage can be interpreted as many things. The most scientifically accurate account measures the Wattage of energy arriving at the skin with a spectrometer, in mW/cm2.
You can also measure the Wattage, as in energy consumption, of panels though, or their rated theoretical Wattage (that's often misleading). For instance, a panel can be rated as 1,500 Watts (theoretical) but only consume 400 Watts of energy when you measure it with a specialized device.
For the most important number, however, check the red light therapy shopping tool to get the mW/cm2 at a 6 inch distance!
This is a post by Bart Wolbers. Bart finished degrees in Physical Therapy (B), Philosophy (BA and MA), Philosophy of Science and Technology (MS - with distinction), and Clinical Health Science (MS), has had training in functional medicine, and is currently chief science writer at Lighttherapyinsiders.com
Found This Interesting? Then You Might Like:
- How To Use Red Light Therapy 101: The Best Guide For Starters
- Red Light Therapy Wavelengths Benefits: The Ultimate Guide
- 36 Powerful Red Light Therapy Benefits
- 18 Science-Backed Systemic Effects Of Red Light Therapy
- Red Light Therapy Dosing Chart: The Raw Data From Hundreds Of Studies
- Red Light Therapy Treatment Protocols: A Startling Revelation
- Red Light Therapy: What’s The Ideal Distance from Skin?
- How Often Should You Use Red Light Therapy Explained







